Blog articles
7/13/23
After the Diagnosis: 7 Ways To Move Forward With an Incurable Disease
by guest writer Rufus Carter
Receiving a diagnosis of a chronic or incurable disease can be an overwhelming and emotional experience. You might feel like your world has been turned upside down and the life you once knew has disappeared. While it may seem difficult, however, it’s possible to move forward and find a new normal. Below, we discuss seven practical steps you can take as you navigate the journey ahead.
1. Grieve and Accept Your Diagnosis
Allowing yourself to grieve and accept your diagnosis is the first step in moving forward. You must acknowledge your feelings and give yourself time to process what has happened. As difficult as it may be, try not to let your diagnosis consume you. Make time for enjoyable activities and surround yourself with loved ones who can offer you genuine support.
2. Learn About Your Disease
Empower yourself with knowledge about your condition. Speak to your doctor about your diagnosis and ask as many questions as necessary to learn about the diagnosis, treatment options, and prognosis. Being well-informed will help you feel more in control and make better decisions about your care.
3. Fine-Tune Your Sleep Habits
Sleep is crucial for our overall health, but it can be hard to come by when coping with an incurable disease. Developing good sleep habits can go a long way toward improving your quality of life. Establish a regular sleep routine, eliminate distractions like electronics, and create a comfortable sleep environment.
When it comes to fostering a healthy sleep environment, consider which investments are worth making. You might be surprised at how impactful new bedding can be for making your bedroom more conducive to sleep and relaxation. These days, you can easily find one-of-a-kind sham designs from artists (consider this option) and have them printed on demand. Whether you opt for patterns to match your sheets and duvet or go with something totally different, you can have a refreshed bed in no time. And since you’re ordering on demand, you can rest assured your design won’t run out of stock.
4. Find Ways To Rest During the Day
If you want to support your energy levels, you must rest as needed during the day. This may mean napping when you feel tired, but it can also mean taking breaks throughout the day to recharge. Sitting in a quiet room, listening to music, or meditating will do wonders for your physical, mental, and emotional health. Listen to your body and do what feels best for you.
5. Engage in Activities You Enjoy
Take time to engage in activities that bring you joy, whether it’s spending time with family, reading a book, or taking on a new hobby. Finding something to look forward to each day can significantly boost your spirits and your mental health. It can also provide a sense of accomplishment and a positive outlook for the future.
6. Manage Your Finances Well
Dealing with medical bills and expenses can be stressful if not overwhelming. You must be able to manage your finances well to avoid such stress. Consider setting up a budget and talking to a financial planner to plan for your future expenses. There might be resources available to help support you financially, but planning ahead is still the best approach.
7. Hire Someone
Adjusting to life with an incurable disease will bring about a wealth of new challenges, and hiring professionals can help you find your stride. Medical professionals like doctors and nurses can provide treatment options and help you manage your symptoms, while mental health professionals such as therapists and counselors can help you cope with the emotional toll of living with your disease. You may also consider hiring a caregiver or home health aide for assistance with daily tasks to improve your overall quality of life.
The Bottom Line
Getting an incurable disease diagnosis is never easy, but remember that you’re not alone. Reach out to friends and family, talk to your healthcare team, foster your mental and physical health, and implement the other strategies above. You will find hope, strength, and inspiration to move forward with your life. Most importantly, see each day as an opportunity to find joy and cherish the time you spend with those who matter most.
After the Diagnosis: 7 Ways To Move Forward With an Incurable Disease
by guest writer Rufus Carter
Receiving a diagnosis of a chronic or incurable disease can be an overwhelming and emotional experience. You might feel like your world has been turned upside down and the life you once knew has disappeared. While it may seem difficult, however, it’s possible to move forward and find a new normal. Below, we discuss seven practical steps you can take as you navigate the journey ahead.
1. Grieve and Accept Your Diagnosis
Allowing yourself to grieve and accept your diagnosis is the first step in moving forward. You must acknowledge your feelings and give yourself time to process what has happened. As difficult as it may be, try not to let your diagnosis consume you. Make time for enjoyable activities and surround yourself with loved ones who can offer you genuine support.
2. Learn About Your Disease
Empower yourself with knowledge about your condition. Speak to your doctor about your diagnosis and ask as many questions as necessary to learn about the diagnosis, treatment options, and prognosis. Being well-informed will help you feel more in control and make better decisions about your care.
3. Fine-Tune Your Sleep Habits
Sleep is crucial for our overall health, but it can be hard to come by when coping with an incurable disease. Developing good sleep habits can go a long way toward improving your quality of life. Establish a regular sleep routine, eliminate distractions like electronics, and create a comfortable sleep environment.
When it comes to fostering a healthy sleep environment, consider which investments are worth making. You might be surprised at how impactful new bedding can be for making your bedroom more conducive to sleep and relaxation. These days, you can easily find one-of-a-kind sham designs from artists (consider this option) and have them printed on demand. Whether you opt for patterns to match your sheets and duvet or go with something totally different, you can have a refreshed bed in no time. And since you’re ordering on demand, you can rest assured your design won’t run out of stock.
4. Find Ways To Rest During the Day
If you want to support your energy levels, you must rest as needed during the day. This may mean napping when you feel tired, but it can also mean taking breaks throughout the day to recharge. Sitting in a quiet room, listening to music, or meditating will do wonders for your physical, mental, and emotional health. Listen to your body and do what feels best for you.
5. Engage in Activities You Enjoy
Take time to engage in activities that bring you joy, whether it’s spending time with family, reading a book, or taking on a new hobby. Finding something to look forward to each day can significantly boost your spirits and your mental health. It can also provide a sense of accomplishment and a positive outlook for the future.
6. Manage Your Finances Well
Dealing with medical bills and expenses can be stressful if not overwhelming. You must be able to manage your finances well to avoid such stress. Consider setting up a budget and talking to a financial planner to plan for your future expenses. There might be resources available to help support you financially, but planning ahead is still the best approach.
7. Hire Someone
Adjusting to life with an incurable disease will bring about a wealth of new challenges, and hiring professionals can help you find your stride. Medical professionals like doctors and nurses can provide treatment options and help you manage your symptoms, while mental health professionals such as therapists and counselors can help you cope with the emotional toll of living with your disease. You may also consider hiring a caregiver or home health aide for assistance with daily tasks to improve your overall quality of life.
The Bottom Line
Getting an incurable disease diagnosis is never easy, but remember that you’re not alone. Reach out to friends and family, talk to your healthcare team, foster your mental and physical health, and implement the other strategies above. You will find hope, strength, and inspiration to move forward with your life. Most importantly, see each day as an opportunity to find joy and cherish the time you spend with those who matter most.
5/31/23
Embracing Change: The Key to Unlocking Personal and Professional Growth
by guest writer Rufus Carter
Embracing change can be a daunting task, but it’s necessary for personal and professional growth. Life is unpredictable, and change is inevitable. Whether you’re starting a new job, moving to a new city, or embarking on a new journey, embracing change can be challenging. However, with the right mindset and positive habits, you can set yourself up for success. Below, Integrative Mental Health Center shares an article on how you can begin to embrace change.
Embrace Evolving Circumstances
Acknowledging and accepting change is the crucial initial step toward embracing it. Although change can be intimidating and uncomfortable, it presents an opportunity for growth and learning. Resisting change will only hinder progress, whereas approaching it with an open mind and positive attitude can lead to success. Therefore, strive to embrace change as a chance for personal and professional development.
Launch Your Enterprise
If you want to take control of your destiny and embrace change, starting your own business is a great option. By pursuing your passions, you can create a brand that aligns with your values and beliefs. To start spreading the word about your venture, make a sharp, eye-catching business card. If you’re not a graphic designer and don’t have the money to hire one, give this tool a look. Customized business cards can help effectively market yourself as an expert in your field, ultimately giving your business the boost it needs to succeed.
Engage In Self-Encouragement
Positive self-talk is a potent tool that empowers you to conquer obstacles and attain your aspirations. By replacing pessimistic thoughts with optimistic ones, and concentrating on your strengths instead of your shortcomings, you can elevate your mindset and attitude. Daily implementation of positive self-talk can bring about a remarkable transformation in your perspective and outlook toward life.
Build Strong, Supportive RelationshipsHaving a supportive network is crucial when it comes to embracing change. You need a group of people who will motivate and encourage you throughout your journey. Look for individuals who are willing to be present for you through thick and thin. Their presence can create a sense of community and belonging that will help you navigate the challenges of change.
Seek a Guiding Mentor
If you're looking to pursue a particular field, having a mentor can be a game-changer. They possess invaluable experience and expertise that can guide and encourage you through life transitions. Don't hesitate to contact someone you admire for advice; finding a mentor can be as simple as that. Once you have a mentor, you'll have a trusted confidant who can offer support and help you achieve your goals.
Monitor and Celebrate Your Accomplishments
Embracing change requires two critical steps - tracking progress and celebrating achievements. These steps are vital, as they keep you motivated and focused on your goals. Consistently setting regular milestones and acknowledging their achievement can provide a sense of accomplishment and much-needed momentum to keep pushing forward. By following this approach, you can guarantee progress and reach your goals with a sense of pride and satisfaction.
Obtain Online Master's Degree Credential
If you're looking to broaden your knowledge and career prospects, taking a look at earning an online master's degree is a must. Pursuing a master's in IT, for instance, can help you stay up-to-date with the latest technology trends and advancements, which in turn, can enable you to open up new job opportunities and command higher salaries. So, if you want to give your career a boost, take a look at the benefits of earning an online master's degree.
Practice Self-Compassion Always
Embracing change requires self-compassion as it can be challenging and bring setbacks. Being kind and patient with yourself throughout the process is vital, and remembering that mistakes should be viewed as opportunities for growth and learning. Cultivating a mindset of self-love and forgiveness is key to managing stress and successfully navigating through changes.
Embracing change is a difficult process that requires self-compassion. It's crucial to be kind, patient, and gentle with yourself throughout the journey, and remember that setbacks and failures are opportunities for growth and learning. Developing a mindset of self-love and forgiveness will help manage the stresses of change and enable successful navigation through it.
Here at Integrative Mental Health Center, we believe that the key to your well-being is a comprehensive approach that addresses your concerns from all angles. Call (480) 426-8040 or use our online scheduler to request an appointment.
Embracing Change: The Key to Unlocking Personal and Professional Growth
by guest writer Rufus Carter
Embracing change can be a daunting task, but it’s necessary for personal and professional growth. Life is unpredictable, and change is inevitable. Whether you’re starting a new job, moving to a new city, or embarking on a new journey, embracing change can be challenging. However, with the right mindset and positive habits, you can set yourself up for success. Below, Integrative Mental Health Center shares an article on how you can begin to embrace change.
Embrace Evolving Circumstances
Acknowledging and accepting change is the crucial initial step toward embracing it. Although change can be intimidating and uncomfortable, it presents an opportunity for growth and learning. Resisting change will only hinder progress, whereas approaching it with an open mind and positive attitude can lead to success. Therefore, strive to embrace change as a chance for personal and professional development.
Launch Your Enterprise
If you want to take control of your destiny and embrace change, starting your own business is a great option. By pursuing your passions, you can create a brand that aligns with your values and beliefs. To start spreading the word about your venture, make a sharp, eye-catching business card. If you’re not a graphic designer and don’t have the money to hire one, give this tool a look. Customized business cards can help effectively market yourself as an expert in your field, ultimately giving your business the boost it needs to succeed.
Engage In Self-Encouragement
Positive self-talk is a potent tool that empowers you to conquer obstacles and attain your aspirations. By replacing pessimistic thoughts with optimistic ones, and concentrating on your strengths instead of your shortcomings, you can elevate your mindset and attitude. Daily implementation of positive self-talk can bring about a remarkable transformation in your perspective and outlook toward life.
Build Strong, Supportive RelationshipsHaving a supportive network is crucial when it comes to embracing change. You need a group of people who will motivate and encourage you throughout your journey. Look for individuals who are willing to be present for you through thick and thin. Their presence can create a sense of community and belonging that will help you navigate the challenges of change.
Seek a Guiding Mentor
If you're looking to pursue a particular field, having a mentor can be a game-changer. They possess invaluable experience and expertise that can guide and encourage you through life transitions. Don't hesitate to contact someone you admire for advice; finding a mentor can be as simple as that. Once you have a mentor, you'll have a trusted confidant who can offer support and help you achieve your goals.
Monitor and Celebrate Your Accomplishments
Embracing change requires two critical steps - tracking progress and celebrating achievements. These steps are vital, as they keep you motivated and focused on your goals. Consistently setting regular milestones and acknowledging their achievement can provide a sense of accomplishment and much-needed momentum to keep pushing forward. By following this approach, you can guarantee progress and reach your goals with a sense of pride and satisfaction.
Obtain Online Master's Degree Credential
If you're looking to broaden your knowledge and career prospects, taking a look at earning an online master's degree is a must. Pursuing a master's in IT, for instance, can help you stay up-to-date with the latest technology trends and advancements, which in turn, can enable you to open up new job opportunities and command higher salaries. So, if you want to give your career a boost, take a look at the benefits of earning an online master's degree.
Practice Self-Compassion Always
Embracing change requires self-compassion as it can be challenging and bring setbacks. Being kind and patient with yourself throughout the process is vital, and remembering that mistakes should be viewed as opportunities for growth and learning. Cultivating a mindset of self-love and forgiveness is key to managing stress and successfully navigating through changes.
Embracing change is a difficult process that requires self-compassion. It's crucial to be kind, patient, and gentle with yourself throughout the journey, and remember that setbacks and failures are opportunities for growth and learning. Developing a mindset of self-love and forgiveness will help manage the stresses of change and enable successful navigation through it.
Here at Integrative Mental Health Center, we believe that the key to your well-being is a comprehensive approach that addresses your concerns from all angles. Call (480) 426-8040 or use our online scheduler to request an appointment.
4/18/23
Just a Few Uses & Interactions of N-Acetyl Cysteine (NAC) in the Brain & Body
by Olivia Valdez, ND
What are Antioxidants?
In the world of naturopathic and alternative medicine, antioxidants boast a large presence for the prevention and mitigation of disease. According to the National Center for Complementary and Integrative Health, an antioxidant is defined as any natural or manmade substance that may prevent or delay some type of cell damage by counteracting oxidative stress (1). Examples of popular antioxidants include Vitamin C, Vitamin E, & beta-carotene, to name just a few. While it is widely accepted that a diet rich in fruits and veggies is beneficial for health and longevity, it is unclear whether this is due to their antioxidant properties or other molecular components. Two powerhouse compounds have been on the forefront of antioxidant research and are demonstrating potential for certain conditions: these are N-acetyl cysteine (NAC) and glutathione (GSH).
NAC is the acetylated version of the amino acid cysteine. Glutathione production is reliant on the amount of NAC that exists in the body at a given time. NAC has been used as an antidote for acetaminophen toxicity. It also as lung tonifying effects, especially as a mucolytic (or mucus-thinning agent). NAC’s parent molecule, GSH, is a tripeptide containing glutamate, glycine, and cysteine and is most active during times of high oxidative stress. Oxidative stress creates radical oxygen species (ROS) in the body, unstable and harmful molecules which can trigger numerous kinds of cell damage (from the formation of atherosclerotic plaque and mitochondrial dysfunction to cell apoptosis) and drive inflammation (2). Oxidative stress actually happens quite frequently and a healthy body can keep these processes in check with its own endogenous antioxidant anti-inflammatory cytokine production. In a body with an excessive load of oxidative stress, however, or one that is immunocompromised, oxidative burden takes over and is then associated in the etiology of many illnesses. NAC and GSH are two of the main mechanisms by which ROSs are eliminated.
In the Brain
NAC has multiple important actions in the brain, not just via its antioxidant effects (its parent, GSH, is the main endogenous antioxidant for the brain), but also its ability to increase neurogenesis, reverse mitochondrial dysfunction, and modulate dopamine and glutamate release (among many others) (3). Psychiatric disorders such as autism spectrum disorder (ASD), obsessive compulsive disorder (OCD), and schizophrenia have their roots in dysregulation of these inflammatory markers, making NAC a promising healing tool.Mixed results were demonstrated from studies with NAC in relation to ASD. In one study, mice with deletions of the chromosome 16p11.2 (which is associated with ASD in humans) demonstrated slowed motor movements, reduced sociability, and a strong anxious disposition when exposed to stress. A single dose of 150 mg/kg of NAC did not regulate the anxiety behaviors but did show benefits in sociability (4). In humans, 5 randomized controlled trials analyzed NAC treatment for ASD in children and adolescents, which were all included in a 2021 meta analysis. The studies lasted 8-24 weeks, included 31-102 participants and utilized an NAC dosage of 500-4200 mg/day. This large study found that NAC significantly improved participants’ Aberrant Behavior Checklist (ABC) scores, irritability, & hyperactivity compared to placebo (5).
OCD is associated with hyperactivity in certain regions of the brain accompanied by an abnormal glutamate metabolism. Increased levels of glutamate can result in excitotoxicity and oxidative stress, which can be found in individuals who suffer from OCD. Results from NAC treatment are mixed here, as well. 5 case reports with an NAC target dose rage of 1800-3000 mg/day demonstrated results from “no effect” to “substantial improvement.” In a 2020 meta analysis which included 5 randomized controlled trials, found NAC significantly improved Yale-Brown Obsessive Compulsive Scale (YBOCS) scores compared to placebo (6). These improvements were not all substantial however, only 2 of which showed at least a 35% reduction (the clinical indication for OCD improvement in patients).NAC may show potential for effective treatment with OCD and OCD-like behaviors, however longer studies are needed to assess delayed effects (especially in relation to long-term mood patterns).
The mechanisms of schizophrenia are still under much scrutiny, but is theorized to be partly characterized by ROS-induced neurotoxicity and apoptotic (cell-killing) pathways (among other etiologies). Magnetic resonance (MR) studies have suggested glutathione reduction and altered glutamate levels in patients with schizophrenia so NAC studies were conducted. In another 2020 meta analysis, 8 weeks of NAC administration (1000-3600 mg/day) had no significant effect on Positive & Negative Syndrome Scale (PANSS) score. But later, at 24 weeks, total and negative PANSS scores were significantly improved compared to placebo along with working memory (7).
In the Pancreas
Elevated levels of glucose and fatty acids (glucolipotoxicity) are two of the main characteristics of diabetes, obesity, and the foundational imbalance of metabolic disorders. These imbalances produce inflammation and destructive and/or toxic effects on pancreatic beta cells, which regulate insulin production in the body and play a key role in glucose homeostasis. Glucolipotoxicity has been shown to be mediated by several other mechanisms, one of which includes GSH metabolism.
In one study examining the effects of pre-administration of NAC on the modulation of oxidative stress in “sick” pancreatic cells, 10 mM’s NAC mitigated the high glucose/high palmitic acid-induced effects of ROS production. GSH levels were also shown to be significantly recovered, although NAC did not restore the pancreatic cell inflammatory response meant to re-balance the body under glucolipotoxicity conditions (8). Another study analyzing the effects of rats with hyperglycemia-induced periodontitis, found that 200mg/kg/day of NAC dissolved in drinking water partially reversed the effect of the high glucose on M1/M2 macrophage polarization (marker of immune response) and therefore ameliorated alveolar (tooth socket) bone loss and osteoclast numbers (9).
Acute pancreatitis, an unfortunate sequalae of moderate to severe hypertriglyceridemia, is partly caused by premature trypsinogen (and other pancreatic enzyme) as well as ROS production –all early signs of pancreatic damage. NAC could be beneficial in preventing the accumulation of pancreatic enzymes and attenuating the ensuing oxidative damage. NAC administration contributed to the down-regulation of cytokines (immune and inflammation mediating proteins) in the early stages of acute pancreatitis (10).
In the Liver
The liver holds chief responsibility for many detoxing and excreting processes along with the synthesis of hormone, cholesterol, and other bodily metabolite pathways. Many exogenous compounds are run through hepatic pathways to be shunted to appropriate tissues of the body or out of the body entirely, these ranging from medications and food substrates to environmental toxins and alcohol. ROS production is commonplace here with this high rate of metabolic activity, and the propensity of inflammatory by-products can be widespread. Even a healthy liver would benefit from intermittent detoxification support and research has suggested NAC can be helpful in mitigating forms of liver pathology, as well.
In a 2022 study testing mice with high fat diet (HFD)-induced fatty liver disease, 2000 mg of NAC daily significantly improved HFD-induced obesity, lipid panel markers, and overall liver health more than placebo. NAC also seemed to “rescue” gut microbiota imbalance caused by the HFD, suggesting benefits for both hepatic and intestinal inflammation (11). A different study focused on acute liver failure which can be caused from a number of drugs, medications, toxins, or even from autoimmune or viral reasons. Due to NAC’s vasodilating, anti-inflammatory, and oxidant-scavenging properties, it may be useful for hepatic pathology regardless of precise causation. In this study, 80 participants diagnosed with non-acetaminophen induced acute liver failure were separated into a continuous IV infusion NAC group of 18.75 mg/kg over a period of three and a half days and a control group. In the NAC group, there was significant improvement found in the survival of patients (mortality rate dropped to 28% from the 53% control group). Additionally, no adverse effects were noted in the NAC administration group, suggesting a high tolerability even in patients with very poor liver function.
Conclusion
So what does all this evidence mean? The studies summarized in this post demonstrate the vast array of health conditions that have potential for decreased morbidity and even healing via NAC (and therefore GSH). This antioxidant has a minimal adverse effect profile (the most common being nausea) and a high tolerability compared to the gold standard medication lines for many of the pathologies discussed above which cannot be characterized this way. And while NAC alone cannot stand as a substitute for any of the principle medications for severe presentations of oxidative stress-induced pathologies, the research is encouraging for its inclusion as an adjunctive treatment for oxidative stress-induced conditions as well as different patient demographics.
Always talk to your doctor about adding any supplementation to your treatment protocol and minimize self-administration. NAC can come in oral forms, injectables, and is even found in certain foods, so a patient-doctor discussion is always a good idea to clarify which kinds of antioxidants and which forms of administration could be more ideal per each unique case. We hope this article was helpful in shedding light on the many purposes of NAC/GSH their potential as an inclusive treatment across many different specialties in the world of naturopathic and alternative medicine.
References
1.https://www.nccih.nih.gov/health/antioxidants-in-depth
2.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8719286/
3.https://link.springer.com/article/10.1007/s40263-022-00907-3
4.https://www.nature.com/articles/s41598-020-69130-8
5.https://doi.org/10.1177%2F0004867420952540
6.https://www.sciencedirect.com/science/article/abs/pii/S2211364920300506?via%3Dihub
7.https://doi.org/10.1177%2F0004867419893439
8.https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0226696
9.https://onlinelibrary.wiley.com/doi/10.1111/jre.12912
10.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3091141/
11.https://pubmed.ncbi.nlm.nih.gov/35229847/
Just a Few Uses & Interactions of N-Acetyl Cysteine (NAC) in the Brain & Body
by Olivia Valdez, ND
What are Antioxidants?
In the world of naturopathic and alternative medicine, antioxidants boast a large presence for the prevention and mitigation of disease. According to the National Center for Complementary and Integrative Health, an antioxidant is defined as any natural or manmade substance that may prevent or delay some type of cell damage by counteracting oxidative stress (1). Examples of popular antioxidants include Vitamin C, Vitamin E, & beta-carotene, to name just a few. While it is widely accepted that a diet rich in fruits and veggies is beneficial for health and longevity, it is unclear whether this is due to their antioxidant properties or other molecular components. Two powerhouse compounds have been on the forefront of antioxidant research and are demonstrating potential for certain conditions: these are N-acetyl cysteine (NAC) and glutathione (GSH).
NAC is the acetylated version of the amino acid cysteine. Glutathione production is reliant on the amount of NAC that exists in the body at a given time. NAC has been used as an antidote for acetaminophen toxicity. It also as lung tonifying effects, especially as a mucolytic (or mucus-thinning agent). NAC’s parent molecule, GSH, is a tripeptide containing glutamate, glycine, and cysteine and is most active during times of high oxidative stress. Oxidative stress creates radical oxygen species (ROS) in the body, unstable and harmful molecules which can trigger numerous kinds of cell damage (from the formation of atherosclerotic plaque and mitochondrial dysfunction to cell apoptosis) and drive inflammation (2). Oxidative stress actually happens quite frequently and a healthy body can keep these processes in check with its own endogenous antioxidant anti-inflammatory cytokine production. In a body with an excessive load of oxidative stress, however, or one that is immunocompromised, oxidative burden takes over and is then associated in the etiology of many illnesses. NAC and GSH are two of the main mechanisms by which ROSs are eliminated.
In the Brain
NAC has multiple important actions in the brain, not just via its antioxidant effects (its parent, GSH, is the main endogenous antioxidant for the brain), but also its ability to increase neurogenesis, reverse mitochondrial dysfunction, and modulate dopamine and glutamate release (among many others) (3). Psychiatric disorders such as autism spectrum disorder (ASD), obsessive compulsive disorder (OCD), and schizophrenia have their roots in dysregulation of these inflammatory markers, making NAC a promising healing tool.Mixed results were demonstrated from studies with NAC in relation to ASD. In one study, mice with deletions of the chromosome 16p11.2 (which is associated with ASD in humans) demonstrated slowed motor movements, reduced sociability, and a strong anxious disposition when exposed to stress. A single dose of 150 mg/kg of NAC did not regulate the anxiety behaviors but did show benefits in sociability (4). In humans, 5 randomized controlled trials analyzed NAC treatment for ASD in children and adolescents, which were all included in a 2021 meta analysis. The studies lasted 8-24 weeks, included 31-102 participants and utilized an NAC dosage of 500-4200 mg/day. This large study found that NAC significantly improved participants’ Aberrant Behavior Checklist (ABC) scores, irritability, & hyperactivity compared to placebo (5).
OCD is associated with hyperactivity in certain regions of the brain accompanied by an abnormal glutamate metabolism. Increased levels of glutamate can result in excitotoxicity and oxidative stress, which can be found in individuals who suffer from OCD. Results from NAC treatment are mixed here, as well. 5 case reports with an NAC target dose rage of 1800-3000 mg/day demonstrated results from “no effect” to “substantial improvement.” In a 2020 meta analysis which included 5 randomized controlled trials, found NAC significantly improved Yale-Brown Obsessive Compulsive Scale (YBOCS) scores compared to placebo (6). These improvements were not all substantial however, only 2 of which showed at least a 35% reduction (the clinical indication for OCD improvement in patients).NAC may show potential for effective treatment with OCD and OCD-like behaviors, however longer studies are needed to assess delayed effects (especially in relation to long-term mood patterns).
The mechanisms of schizophrenia are still under much scrutiny, but is theorized to be partly characterized by ROS-induced neurotoxicity and apoptotic (cell-killing) pathways (among other etiologies). Magnetic resonance (MR) studies have suggested glutathione reduction and altered glutamate levels in patients with schizophrenia so NAC studies were conducted. In another 2020 meta analysis, 8 weeks of NAC administration (1000-3600 mg/day) had no significant effect on Positive & Negative Syndrome Scale (PANSS) score. But later, at 24 weeks, total and negative PANSS scores were significantly improved compared to placebo along with working memory (7).
In the Pancreas
Elevated levels of glucose and fatty acids (glucolipotoxicity) are two of the main characteristics of diabetes, obesity, and the foundational imbalance of metabolic disorders. These imbalances produce inflammation and destructive and/or toxic effects on pancreatic beta cells, which regulate insulin production in the body and play a key role in glucose homeostasis. Glucolipotoxicity has been shown to be mediated by several other mechanisms, one of which includes GSH metabolism.
In one study examining the effects of pre-administration of NAC on the modulation of oxidative stress in “sick” pancreatic cells, 10 mM’s NAC mitigated the high glucose/high palmitic acid-induced effects of ROS production. GSH levels were also shown to be significantly recovered, although NAC did not restore the pancreatic cell inflammatory response meant to re-balance the body under glucolipotoxicity conditions (8). Another study analyzing the effects of rats with hyperglycemia-induced periodontitis, found that 200mg/kg/day of NAC dissolved in drinking water partially reversed the effect of the high glucose on M1/M2 macrophage polarization (marker of immune response) and therefore ameliorated alveolar (tooth socket) bone loss and osteoclast numbers (9).
Acute pancreatitis, an unfortunate sequalae of moderate to severe hypertriglyceridemia, is partly caused by premature trypsinogen (and other pancreatic enzyme) as well as ROS production –all early signs of pancreatic damage. NAC could be beneficial in preventing the accumulation of pancreatic enzymes and attenuating the ensuing oxidative damage. NAC administration contributed to the down-regulation of cytokines (immune and inflammation mediating proteins) in the early stages of acute pancreatitis (10).
In the Liver
The liver holds chief responsibility for many detoxing and excreting processes along with the synthesis of hormone, cholesterol, and other bodily metabolite pathways. Many exogenous compounds are run through hepatic pathways to be shunted to appropriate tissues of the body or out of the body entirely, these ranging from medications and food substrates to environmental toxins and alcohol. ROS production is commonplace here with this high rate of metabolic activity, and the propensity of inflammatory by-products can be widespread. Even a healthy liver would benefit from intermittent detoxification support and research has suggested NAC can be helpful in mitigating forms of liver pathology, as well.
In a 2022 study testing mice with high fat diet (HFD)-induced fatty liver disease, 2000 mg of NAC daily significantly improved HFD-induced obesity, lipid panel markers, and overall liver health more than placebo. NAC also seemed to “rescue” gut microbiota imbalance caused by the HFD, suggesting benefits for both hepatic and intestinal inflammation (11). A different study focused on acute liver failure which can be caused from a number of drugs, medications, toxins, or even from autoimmune or viral reasons. Due to NAC’s vasodilating, anti-inflammatory, and oxidant-scavenging properties, it may be useful for hepatic pathology regardless of precise causation. In this study, 80 participants diagnosed with non-acetaminophen induced acute liver failure were separated into a continuous IV infusion NAC group of 18.75 mg/kg over a period of three and a half days and a control group. In the NAC group, there was significant improvement found in the survival of patients (mortality rate dropped to 28% from the 53% control group). Additionally, no adverse effects were noted in the NAC administration group, suggesting a high tolerability even in patients with very poor liver function.
Conclusion
So what does all this evidence mean? The studies summarized in this post demonstrate the vast array of health conditions that have potential for decreased morbidity and even healing via NAC (and therefore GSH). This antioxidant has a minimal adverse effect profile (the most common being nausea) and a high tolerability compared to the gold standard medication lines for many of the pathologies discussed above which cannot be characterized this way. And while NAC alone cannot stand as a substitute for any of the principle medications for severe presentations of oxidative stress-induced pathologies, the research is encouraging for its inclusion as an adjunctive treatment for oxidative stress-induced conditions as well as different patient demographics.
Always talk to your doctor about adding any supplementation to your treatment protocol and minimize self-administration. NAC can come in oral forms, injectables, and is even found in certain foods, so a patient-doctor discussion is always a good idea to clarify which kinds of antioxidants and which forms of administration could be more ideal per each unique case. We hope this article was helpful in shedding light on the many purposes of NAC/GSH their potential as an inclusive treatment across many different specialties in the world of naturopathic and alternative medicine.
References
1.https://www.nccih.nih.gov/health/antioxidants-in-depth
2.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8719286/
3.https://link.springer.com/article/10.1007/s40263-022-00907-3
4.https://www.nature.com/articles/s41598-020-69130-8
5.https://doi.org/10.1177%2F0004867420952540
6.https://www.sciencedirect.com/science/article/abs/pii/S2211364920300506?via%3Dihub
7.https://doi.org/10.1177%2F0004867419893439
8.https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0226696
9.https://onlinelibrary.wiley.com/doi/10.1111/jre.12912
10.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3091141/
11.https://pubmed.ncbi.nlm.nih.gov/35229847/
2/1/23
Candidiasis – A Potential Post-Holiday Pathos
by Olivia Valdez, ND
We have finally reached the New Year, with the holidays slowly receding in our rear-view mirror. Hopefully we connected with loved ones, enjoyed some time away from major responsibilities, and indulged in our favorite treats. Healthy feasting is only appropriate during this time, after all! But now that we’re starting over again, giving our bodies a rest from the carbohydrates and sugar can help prevent one type of gastrointestinal (GI) flora imbalance –candidiasis, or most commonly an overgrowth of Candida albicans, a naturally-occurring type of fungus [1]. While we all have innate quantities of this organism living inside us in our mouths, skin, and intestines, when C. albicans becomes overgrown, it can cause a host of unwanted physical and even mental/emotional symptoms. But first, let’s get some background on where C. albicans comes from.
The microbiome is defined as the collection of all microbes, such as bacteria, fungi, viruses, and their genes, that natural live on our bodies and inside of us and is first established during infancy [2]. This article will focus mainly on the microbiome that exists in our GI tract and how C. albicans is just one community living in the major metropolitan area that is our intestines and colon. A healthy gut microbiome has a wholesome balance of different microbes that work synergistically for our benefit. These microbes can send alarm signals to your immune system when threatened, break down toxic food compounds that threaten the integrity of your gut lining, and synthesize certain vitamins and amino acids for your brain and metabolic health (among many, many other roles) [3]. The goal of current microbiome researchers is to map a “typical”, from a Western society, human gut ecosystem, with acknowledgement that there will be standard deviations between people of different cultures and ages. One of the most important, delineating factors that shapes a gut microbiome is what you feed it – yes, the food you put in your mouth that travels all the way down this ecosystem and feeds all the inhabitants—whether it be an In N Out double-double with fries or a homemade vegetable stew. When you eat, your microbes eat too and this is where nutrition quality affects how your microbiome is constituted: feed the happy microbes, the beneficial ones, and boast a clear-headed mindset and an energized metabolism. Feed the microbes that are prone to anger, the opportunistic or pathogenic ones, and begin to suffer early signs of chronic illnesses like high blood sugar, chronic fatigue, and joint pain [4]. Our friend from the introduction, C. albicans, falls into the opportunistic category: happy when in appropriate amounts and angry when overgrown.
In a healthy individual with a balanced microbiome, C. albicans has been postulated to be skilled at “educating” our immune system. Intestinal C. albicans colonization can induce an innate immune memory called trained immunity and helps in shaping T-cell responses, especially Th17, which is very important for gut lining strength and prevention of leaky gut. Leaky gut is a condition in which a porous intestinal wall allows food and other toxic molecules to cross it when it should not [5]. In other words, its intestinal presence allows our immune system to recognize C. albicans and limit its presence to inside the gut by strengthening its walls, preventing it from spreading into the bloodstream, which would be problematic for the rest of our body!. Additionally, there is empirical evidence supporting the idea that intestinal C. albicans helps keep other opportunistic microbes in check: Staphylococcus aureus, Aspergillus fumigatus, and Pseudomonas aeruginosa being a few examples [5]. But when a poor diet, a suppressed immune system, and/or a defective gut lining causes C. albicans to flare and spread, the tides turn and it begins to wreak havoc both in and outside our microbiome. Crohn’s disease, ulcerative colitis, and the formation of gastric ulcers have all been associated with an overgrowth of C. albicans, which in turn, emits toxic byproducts like acetaldehyde, ammonia, & uric acid, and triggers flares in other kinds of opportunistic and pathogenic microbes [6]. These byproducts can travel the length of the intestines, creating gas and bloating, diarrhea and/or constipation, abdominal cramps, and nausea. As they slip out of a porous gut lining and travel into the bloodstream, headaches, joint pain, brain fog, confusion, memory impairment, mood changes, and even other opportunistic infections can ensue. Too much C. albicans can deplete you of certain vitamins, amino acids, and neurotransmitters, as well. Fatty acids, iron, magnesium, and Vit B6 which are stolen and destroyed by C. albicans can contribute to chronic fatigue and malnutrition. Similarly, suppressed production of serotonin, dopamine, and B12 lead to a range of mental health symptoms such as depression, anxiety, and a labile mood (which can falsely mimic other conditions such as bipolar or borderline personality disorder [BPD] [7].
So how can we keep C. albicans in check? In addition to keeping antibiotics and stress levels to a minimum, we do not want to overfeed it. C. albicans dines on simple carbohydrates and sugar so the key to its discipline is providing it with a glucose and fructose-limited environment [8]. Much of the standard American diet (SAD) is loaded with C. albicans favorite foods: French fries, cakes, cookies, pasta, pizza, candy, bread, and soda. To avoid C. albicans proliferation, using food as medicine and cultivating a dietary lifestyle that consists of a whole foods diet that consists mainly of vegetables, proteins, low-glycemic fruits, and healthy fats is the goal. Fiber from vegetables such as leafy greens provide prebiotics for good microbes to better balance opportunistic ones. Healthy fats such as avocados, nuts & seeds, and extra virgin olive oil are broken down into short chain fatty acids (SCFAs) which help drive your energy and metabolism but are essentially useless for C. albicans’ [9]. Eating sufficient protein (from sources such as grass-fed beef, wild-caught fish, and organic poultry) regulate satiety mechanisms so you feel less inclined to reach for the bag of popcorn or the last handful of chips. Appropriate protein quantities also tell your gut and its microbes where they are in the timeline of your feeding cycles—a useful piece of information for portion management and balancing feasting and fasting processes.
If a C. albicans proliferation is extremely strong, sometimes a more restrictive nutrition protocol is needed for a period of 3-6 months. This would include eliminating most grains, many types of fruit, dairy products and fermented foods which contain natural sources of yeast and/or simple sugars. When we work with patients who have a strong C. albicans presentation, we often also use antimicrobial supplements and herbs to pair with the nutrition. Mimicking Nystatin, herbs such as Juglans nigra (Black Walnut) and Origanum vulgare (Oregano) can directly target and kill C. albicans, decreasing the overgrowth. With these heavy hitters, we always inform patients of the importance of hydration and maintenance of daily bowel movements so the die-off may be flushed out as quickly and efficiently as possible. Supplements such as activated charcoal can help bind up the dead C. albicans and escort it safely out of the body through the colon. With good compliance, a patient may see an improvement in their symptoms within 1-3 months of beginning this protocol. At that point, the last phase of treatment aims to heal and strengthen the gut environment, preventing future proliferations of opportunistic species. Drinking daily bone broth, the addition of glutamine powder, intermittent fasting, topical castor oil packs, and the use of carminative herbs can all be useful treatments in the healing phase of a C. albicans protocol. Choosing the right combination of treatments depends on a patient’s past medical history and the presence of any comorbid conditions – this is best discussed in collaboration with your ND.
In conclusion, at IMHC, we know it is important to rest and celebrate to the fullest with our loved ones—to feast and have fun with minimal worry about things like gut microbes and weird yeast issues. After all, life should be lived in balance. And we also know that it is just as important to return to daily activities with a sense mental peace and clarity. We hope this article sheds some light on how you can ease this return to your life as you embark into a new year. May it bring all the unique potential you wish for and may you and your microbes be happy and well-fed.
Peace, love, & Lactobacillus (that’s the good stuff).
References
Candidiasis – A Potential Post-Holiday Pathos
by Olivia Valdez, ND
We have finally reached the New Year, with the holidays slowly receding in our rear-view mirror. Hopefully we connected with loved ones, enjoyed some time away from major responsibilities, and indulged in our favorite treats. Healthy feasting is only appropriate during this time, after all! But now that we’re starting over again, giving our bodies a rest from the carbohydrates and sugar can help prevent one type of gastrointestinal (GI) flora imbalance –candidiasis, or most commonly an overgrowth of Candida albicans, a naturally-occurring type of fungus [1]. While we all have innate quantities of this organism living inside us in our mouths, skin, and intestines, when C. albicans becomes overgrown, it can cause a host of unwanted physical and even mental/emotional symptoms. But first, let’s get some background on where C. albicans comes from.
The microbiome is defined as the collection of all microbes, such as bacteria, fungi, viruses, and their genes, that natural live on our bodies and inside of us and is first established during infancy [2]. This article will focus mainly on the microbiome that exists in our GI tract and how C. albicans is just one community living in the major metropolitan area that is our intestines and colon. A healthy gut microbiome has a wholesome balance of different microbes that work synergistically for our benefit. These microbes can send alarm signals to your immune system when threatened, break down toxic food compounds that threaten the integrity of your gut lining, and synthesize certain vitamins and amino acids for your brain and metabolic health (among many, many other roles) [3]. The goal of current microbiome researchers is to map a “typical”, from a Western society, human gut ecosystem, with acknowledgement that there will be standard deviations between people of different cultures and ages. One of the most important, delineating factors that shapes a gut microbiome is what you feed it – yes, the food you put in your mouth that travels all the way down this ecosystem and feeds all the inhabitants—whether it be an In N Out double-double with fries or a homemade vegetable stew. When you eat, your microbes eat too and this is where nutrition quality affects how your microbiome is constituted: feed the happy microbes, the beneficial ones, and boast a clear-headed mindset and an energized metabolism. Feed the microbes that are prone to anger, the opportunistic or pathogenic ones, and begin to suffer early signs of chronic illnesses like high blood sugar, chronic fatigue, and joint pain [4]. Our friend from the introduction, C. albicans, falls into the opportunistic category: happy when in appropriate amounts and angry when overgrown.
In a healthy individual with a balanced microbiome, C. albicans has been postulated to be skilled at “educating” our immune system. Intestinal C. albicans colonization can induce an innate immune memory called trained immunity and helps in shaping T-cell responses, especially Th17, which is very important for gut lining strength and prevention of leaky gut. Leaky gut is a condition in which a porous intestinal wall allows food and other toxic molecules to cross it when it should not [5]. In other words, its intestinal presence allows our immune system to recognize C. albicans and limit its presence to inside the gut by strengthening its walls, preventing it from spreading into the bloodstream, which would be problematic for the rest of our body!. Additionally, there is empirical evidence supporting the idea that intestinal C. albicans helps keep other opportunistic microbes in check: Staphylococcus aureus, Aspergillus fumigatus, and Pseudomonas aeruginosa being a few examples [5]. But when a poor diet, a suppressed immune system, and/or a defective gut lining causes C. albicans to flare and spread, the tides turn and it begins to wreak havoc both in and outside our microbiome. Crohn’s disease, ulcerative colitis, and the formation of gastric ulcers have all been associated with an overgrowth of C. albicans, which in turn, emits toxic byproducts like acetaldehyde, ammonia, & uric acid, and triggers flares in other kinds of opportunistic and pathogenic microbes [6]. These byproducts can travel the length of the intestines, creating gas and bloating, diarrhea and/or constipation, abdominal cramps, and nausea. As they slip out of a porous gut lining and travel into the bloodstream, headaches, joint pain, brain fog, confusion, memory impairment, mood changes, and even other opportunistic infections can ensue. Too much C. albicans can deplete you of certain vitamins, amino acids, and neurotransmitters, as well. Fatty acids, iron, magnesium, and Vit B6 which are stolen and destroyed by C. albicans can contribute to chronic fatigue and malnutrition. Similarly, suppressed production of serotonin, dopamine, and B12 lead to a range of mental health symptoms such as depression, anxiety, and a labile mood (which can falsely mimic other conditions such as bipolar or borderline personality disorder [BPD] [7].
So how can we keep C. albicans in check? In addition to keeping antibiotics and stress levels to a minimum, we do not want to overfeed it. C. albicans dines on simple carbohydrates and sugar so the key to its discipline is providing it with a glucose and fructose-limited environment [8]. Much of the standard American diet (SAD) is loaded with C. albicans favorite foods: French fries, cakes, cookies, pasta, pizza, candy, bread, and soda. To avoid C. albicans proliferation, using food as medicine and cultivating a dietary lifestyle that consists of a whole foods diet that consists mainly of vegetables, proteins, low-glycemic fruits, and healthy fats is the goal. Fiber from vegetables such as leafy greens provide prebiotics for good microbes to better balance opportunistic ones. Healthy fats such as avocados, nuts & seeds, and extra virgin olive oil are broken down into short chain fatty acids (SCFAs) which help drive your energy and metabolism but are essentially useless for C. albicans’ [9]. Eating sufficient protein (from sources such as grass-fed beef, wild-caught fish, and organic poultry) regulate satiety mechanisms so you feel less inclined to reach for the bag of popcorn or the last handful of chips. Appropriate protein quantities also tell your gut and its microbes where they are in the timeline of your feeding cycles—a useful piece of information for portion management and balancing feasting and fasting processes.
If a C. albicans proliferation is extremely strong, sometimes a more restrictive nutrition protocol is needed for a period of 3-6 months. This would include eliminating most grains, many types of fruit, dairy products and fermented foods which contain natural sources of yeast and/or simple sugars. When we work with patients who have a strong C. albicans presentation, we often also use antimicrobial supplements and herbs to pair with the nutrition. Mimicking Nystatin, herbs such as Juglans nigra (Black Walnut) and Origanum vulgare (Oregano) can directly target and kill C. albicans, decreasing the overgrowth. With these heavy hitters, we always inform patients of the importance of hydration and maintenance of daily bowel movements so the die-off may be flushed out as quickly and efficiently as possible. Supplements such as activated charcoal can help bind up the dead C. albicans and escort it safely out of the body through the colon. With good compliance, a patient may see an improvement in their symptoms within 1-3 months of beginning this protocol. At that point, the last phase of treatment aims to heal and strengthen the gut environment, preventing future proliferations of opportunistic species. Drinking daily bone broth, the addition of glutamine powder, intermittent fasting, topical castor oil packs, and the use of carminative herbs can all be useful treatments in the healing phase of a C. albicans protocol. Choosing the right combination of treatments depends on a patient’s past medical history and the presence of any comorbid conditions – this is best discussed in collaboration with your ND.
In conclusion, at IMHC, we know it is important to rest and celebrate to the fullest with our loved ones—to feast and have fun with minimal worry about things like gut microbes and weird yeast issues. After all, life should be lived in balance. And we also know that it is just as important to return to daily activities with a sense mental peace and clarity. We hope this article sheds some light on how you can ease this return to your life as you embark into a new year. May it bring all the unique potential you wish for and may you and your microbes be happy and well-fed.
Peace, love, & Lactobacillus (that’s the good stuff).
References
- https://my.clevelandclinic.org/health/diseases/22961-candida-albicans
- https://www.niehs.nih.gov/health/topics/science/microbiome/index.cfm
- https://www.hsph.harvard.edu/nutritionsource/microbiome/
- https://www.otsuka.co.jp/en/health-and-illness/fiber/for-body/intestinal-flora/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7744392/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3163673/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4955731/
- https://www.frontiersin.org/articles/10.3389/fmicb.2019.00099/full
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7744392/
12/15/22
Feeling Disordered – The Season
by Olivia Valdez, ND
As the summer months shift to fall and winter, the days become shorter and the nights become longer. The sun moves further away from Earth and the daylight becomes seemingly more elusive. This natural cycle can leave us feeling less motivated and more prone to depression—a combination of biologic and mood disturbances referred to as seasonal affective disorder (SAD) [1]. And though it occurs more commonly at the onset of fall and winter, it may also flare during other times of the year. Community-based studies estimate that the prevalence of SAD is close to 10% in northern latitudes (in Canada & the US combined, for example) and predominates more in women than men (by a ratio of 4:1, respectively) [2].
According to the literature, SAD has multiple factors attributed to its etiology but mainly appears as a result of changes to our natural circadian rhythms. Almost all biological creatures have this rhythm which regulates the physical, mental, and behavioral changes correlating to light and dark over a 24-hour period [3]. Circadian rhythms affect our health by releasing hormones, regulating our eating habits & digestion, and modulating body temperature all in correspondence to the time of day or night we are in. In SAD, a phase delay of our circadian rhythm relative to our sleep/wake cycle is postulated to be at the root of winter depression. This theory is called the Phase Shift Hypothesis (PSH) and is the leading philosophy behind SAD. In order to identify circadian phase position in humans, salivary dim light melatonin onset (DLMO) is utilized as a marker [4]. Melatonin is the hormone secreted from the pineal gland in the brain which modulates sleep-wake cycles (among its other roles). In dimly lit environments, melatonin is actively secreted and in bright-light environments, it is suppressed. So how does this all tie together? In order to correct phase delays which cause SAD, correctly timed low-dose melatonin and exposure to bright light can bring the misalignments back into homeostasis and improve emotional wellbeing. And as it currently stands, light therapy has proven to be one of the most effective treatments for SAD.
SAD can have many overlapping symptoms with major depressive disorder (MDD) and is even classified under the umbrella of MDD. The difference, however, is that SAD is characterized by a seasonal pattern and must outnumber the nonseasonal major depressive episodes that may have occurred over a person’s lifetime [1]. Oversleeping (hypersomnia), overeating (especially carbohydrates), weight gain, and social withdrawal (feeling like you want to hibernate) are all commonplace experiences. The bright side of SAD is recognizing your body has an innate awareness of its position in time – realizing there is an evidence-based cause for the way you feel and knowing there was nothing you did wrong. So how can you support yourself the most during fall and winter? What extra TLC might your mind and body thank you for this month?
Our winter wellness tools are many-fold and at IMHC and we can help you find the right combination of treatments for the most alleviation from SAD. The first therapy to consider is a light lamp. This apparatus mimic’s the rays of the sun and can bring you 10,000 lux of light filtered through an ultraviolet shield. Turning this on and sitting in front of it for 15-30 mins upon waking can help suppress the hormone melatonin and boost feelings of wakefulness and drive [5]. Some lamps have dim settings for evening, as well, which can help balance morning brightness with evening “sunset.” Targeted supplementation can also help balance neurotransmitters and hormones associated with mood. Our favorite nutraceuticals to recommend for SAD include high dose Vitamin D & low dose 5-HTP as well as adaptogenic, naturally uplifting herbs such as Rhodiola rosea and Eleutherococcus senticosus. The latter two are preferentially dosed before 2pm to avoid overstimulation close to bedtime, which is another tip of the hat to a healthy circadian rhythm. With varying mechanisms of action, these compounds work to support your body’s metabolic processes while also stabilizing the mental/emotional state. The other wonderful option for SAD includes homeopathy – this medicine not only helps soothe the nervous system and strengthen resilience in someone with SAD, but improves overall quality of life so they can function efficiently and still tackle their daily activities with minimal interference from fatigue and depression.
Lifestyle can also play an impactful role in SAD. What you eat, when you move, and who you interact with all have a part to play in alleviating feelings of depression and optimizing wellness and vitality, especially during the winter months. Eating cooked foods over raw is preferable, as they are more energetically warming. You can take this further by even cooking your proteins and veggies in warming spices like ginger, turmeric, cinnamon, clove, cumin, & black pepper. Combining this nutrition style with gentle exercise of any kind can keep your body happy and warm through this time. Dancing, online exercise videos, swimming (in a mildly heated pool), biking, walking, and yoga can all support healthy serotonin, dopamine, & endocrine hormone production such as epinephrine & norepinephrine (and these are just a few examples). One of the last (but definitely not least) aspects to consider when treating SAD is maintaining connection and community. Being around others helps combat intrusive and negative thought patterns by providing both a distraction and replacement with positive, external experiences [6]. One of the best medicines for SAD can be feeling valued, comfortable, and safe within an close or intimate social circle. If you gather around a fire with friends, share a warm meal, and remind each other to take your Vitamin D, you will be mirroring how human beings have passed the winter months since the beginning of time. In a moment like this, it is much more difficult to feel disordered.
Our team at IMHC can help you identify if you are being affected by SAD and guide you in finding the tools you need to feel your best during the season. We recognize that each person has a unique constitution and what works for one person may be completely different from what works for another. If any of the above messages have resonated with you, know that you are not alone and that there are many reasons and resources for optimism. Healing is a learning curve and we are here to guide you along it. Stop by our office in Scottsdale for your individualized naturopathic support!
References
Feeling Disordered – The Season
by Olivia Valdez, ND
As the summer months shift to fall and winter, the days become shorter and the nights become longer. The sun moves further away from Earth and the daylight becomes seemingly more elusive. This natural cycle can leave us feeling less motivated and more prone to depression—a combination of biologic and mood disturbances referred to as seasonal affective disorder (SAD) [1]. And though it occurs more commonly at the onset of fall and winter, it may also flare during other times of the year. Community-based studies estimate that the prevalence of SAD is close to 10% in northern latitudes (in Canada & the US combined, for example) and predominates more in women than men (by a ratio of 4:1, respectively) [2].
According to the literature, SAD has multiple factors attributed to its etiology but mainly appears as a result of changes to our natural circadian rhythms. Almost all biological creatures have this rhythm which regulates the physical, mental, and behavioral changes correlating to light and dark over a 24-hour period [3]. Circadian rhythms affect our health by releasing hormones, regulating our eating habits & digestion, and modulating body temperature all in correspondence to the time of day or night we are in. In SAD, a phase delay of our circadian rhythm relative to our sleep/wake cycle is postulated to be at the root of winter depression. This theory is called the Phase Shift Hypothesis (PSH) and is the leading philosophy behind SAD. In order to identify circadian phase position in humans, salivary dim light melatonin onset (DLMO) is utilized as a marker [4]. Melatonin is the hormone secreted from the pineal gland in the brain which modulates sleep-wake cycles (among its other roles). In dimly lit environments, melatonin is actively secreted and in bright-light environments, it is suppressed. So how does this all tie together? In order to correct phase delays which cause SAD, correctly timed low-dose melatonin and exposure to bright light can bring the misalignments back into homeostasis and improve emotional wellbeing. And as it currently stands, light therapy has proven to be one of the most effective treatments for SAD.
SAD can have many overlapping symptoms with major depressive disorder (MDD) and is even classified under the umbrella of MDD. The difference, however, is that SAD is characterized by a seasonal pattern and must outnumber the nonseasonal major depressive episodes that may have occurred over a person’s lifetime [1]. Oversleeping (hypersomnia), overeating (especially carbohydrates), weight gain, and social withdrawal (feeling like you want to hibernate) are all commonplace experiences. The bright side of SAD is recognizing your body has an innate awareness of its position in time – realizing there is an evidence-based cause for the way you feel and knowing there was nothing you did wrong. So how can you support yourself the most during fall and winter? What extra TLC might your mind and body thank you for this month?
Our winter wellness tools are many-fold and at IMHC and we can help you find the right combination of treatments for the most alleviation from SAD. The first therapy to consider is a light lamp. This apparatus mimic’s the rays of the sun and can bring you 10,000 lux of light filtered through an ultraviolet shield. Turning this on and sitting in front of it for 15-30 mins upon waking can help suppress the hormone melatonin and boost feelings of wakefulness and drive [5]. Some lamps have dim settings for evening, as well, which can help balance morning brightness with evening “sunset.” Targeted supplementation can also help balance neurotransmitters and hormones associated with mood. Our favorite nutraceuticals to recommend for SAD include high dose Vitamin D & low dose 5-HTP as well as adaptogenic, naturally uplifting herbs such as Rhodiola rosea and Eleutherococcus senticosus. The latter two are preferentially dosed before 2pm to avoid overstimulation close to bedtime, which is another tip of the hat to a healthy circadian rhythm. With varying mechanisms of action, these compounds work to support your body’s metabolic processes while also stabilizing the mental/emotional state. The other wonderful option for SAD includes homeopathy – this medicine not only helps soothe the nervous system and strengthen resilience in someone with SAD, but improves overall quality of life so they can function efficiently and still tackle their daily activities with minimal interference from fatigue and depression.
Lifestyle can also play an impactful role in SAD. What you eat, when you move, and who you interact with all have a part to play in alleviating feelings of depression and optimizing wellness and vitality, especially during the winter months. Eating cooked foods over raw is preferable, as they are more energetically warming. You can take this further by even cooking your proteins and veggies in warming spices like ginger, turmeric, cinnamon, clove, cumin, & black pepper. Combining this nutrition style with gentle exercise of any kind can keep your body happy and warm through this time. Dancing, online exercise videos, swimming (in a mildly heated pool), biking, walking, and yoga can all support healthy serotonin, dopamine, & endocrine hormone production such as epinephrine & norepinephrine (and these are just a few examples). One of the last (but definitely not least) aspects to consider when treating SAD is maintaining connection and community. Being around others helps combat intrusive and negative thought patterns by providing both a distraction and replacement with positive, external experiences [6]. One of the best medicines for SAD can be feeling valued, comfortable, and safe within an close or intimate social circle. If you gather around a fire with friends, share a warm meal, and remind each other to take your Vitamin D, you will be mirroring how human beings have passed the winter months since the beginning of time. In a moment like this, it is much more difficult to feel disordered.
Our team at IMHC can help you identify if you are being affected by SAD and guide you in finding the tools you need to feel your best during the season. We recognize that each person has a unique constitution and what works for one person may be completely different from what works for another. If any of the above messages have resonated with you, know that you are not alone and that there are many reasons and resources for optimism. Healing is a learning curve and we are here to guide you along it. Stop by our office in Scottsdale for your individualized naturopathic support!
References
- https://www.aafp.org/pubs/afp/issues/2012/1201/p1037.html
- https://www.nimh.nih.gov/health/publications/seasonal-affective-disorder
- https://nigms.nih.gov/education/fact-sheets/Pages/circadian-rhythms.aspx
- https://www.researchgate.net/publication/5876179_The_phase_shift_hypothesis_for_the_circadian_component_of_winter_depression
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5934317/
- https://www.headtohealth.gov.au/meaningful-life/connectedness/community
8/31/22
Could Your Anxiety Be Related to Progesterone Levels? By Tara Peyman, ND
Anxiety is one of the most common mental health conditions. Feelings of anxiousness are normal for everyone to experience from time to time. However, for some people, anxiety can become severe and interruptive to daily functioning. This is when it is important to seek professional help and look for the underlying cause.
Sometimes anxiety is related to ongoing stress in your current daily life, and sometimes there is a history of trauma that has wired your nervous system to get stuck in a fight or flight state, leading to persistent anxiety even when there is nothing externally wrong in your current life to cause such high levels of anxiety. Stress and trauma tend to respond well to psychological therapy, such as CBT, EMDR, or other counseling modalities. Some people get great relief using natural supplements for stress reduction, such as passionflower, L-theanine, or homeopathic remedies.
Yet sometimes there is another cause. For females with anxiety, there can be a hormonal connection. If you notice that anxiety levels tend to fluctuate throughout the month, or if anxiety has been worse since menopausal changes, hormones may be at play here.
Progesterone can have a tranquilizing effect on the brain and nervous system. It does this primarily by acting on GABA receptors to calm the body and brain.1,2 Interestingly, there is a gut-brain connection with progesterone as well. Progesterone has been found to act as a probiotic in the digestive system, promoting growth of the beneficial bacteria, lactobacillus reuteri.3 This healthy bacteria strain has been shown to diminish anxiety levels and improve mental health.
If progesterone levels are relatively low, the nervous system may feel more stimulated, anxious, and restless. Some females with low progesterone will feel highly irritable as well. Low progesterone may lead to insomnia, which often happens during the luteal phase of a woman’s menstrual cycle, the phase when PMS is most likely to occur.
Progesterone also tends to drop first, before estrogen levels drop, during perimenopause. This means that females in their 40s and early 50s may start to have difficulty with insomnia, irritability, and anxiety, before they develop the classic menopausal symptoms of hot flashes and night sweats, which are more commonly related to a drop in estrogen.
If you are curious about whether progesterone might be a contributing factor in your anxiety, one good first step would be to make some notes about when anxiety occurs. Does there seem to be a cyclical pattern of anxiety or agitation increasing before your menstrual cycle? Has anxiety or insomnia increased or started as you’ve gotten older, possibly related to declining progesterone levels?
Most of the time, there are multiple factors that lead to heightened anxiety, and these factors play off of each other. For example, if your progesterone is lower, and you are not sleeping well and feeling anxious, you may be less productive at work or more irritable with others, and this can lead to increased stress and worry about these issues.
Stress and anxiety also can play a role in reducing progesterone levels, because progesterone is partly produced by the adrenal glands, and when you are under greater stress, your adrenal glands – the primary glands responsible for stress management in the body – will shunt more of their focus to production of cortisol and reduce focus on reproductive hormone production. So, in this way, there can be a cyclical effect of stress and anxiety causing low progesterone, which leads to more anxiety and stress.
How can we intervene to help this problem? Hormone testing is the first key element, to measure your levels of progesterone, estrogen, testosterone, cortisol, DHEA, thyroid hormones, vitamin D, and other markers that your doctor might be interested in testing, to get the whole picture of your internal health status. Once you have test results, your doctor can help determine whether there are imbalances between your hormones, or other issues that need to be addressed, in order to resolve the issues you are facing.
Treatment for progesterone deficiency may include herbal supplements, such as vitex, to promote more progesterone effects in the body. Vitex can also have specific antidepressant and anti-anxiety benefits, in addition to its hormone balancing effects, and was found to be similar in efficacy to fluoxetine in one study.4 If estrogen is relatively high and progesterone is normal or only slightly suboptimal, bringing the ratio into balance is key. This can be done with an estrogen reducing natural supplement, such as DIM (diindolylmethane) or I3C (indole-3-carbanol), both made from vegetable sources. For people with very low progesterone, or women further into perimenopause, progesterone supplementation may be a better option. This can take the form of low dose over-the-counter progesterone creams, or a bioidentical progesterone prescription from a pharmacy.
It is important to be well informed regarding all the risks and benefits of these treatment options, and to discuss them in detail with a doctor who is well versed in holistic hormone treatments. It is also vital to focus on the whole picture, because when it comes to hormonal health, balance is key. What is most important is to have the right ratios of each of the hormones, as well as a healthy diet and lifestyle that includes mindful self-care, to feel at your best.
References:
1. Antonia V. Seligowski, et al., Translational studies of estradiol and progesterone in fear and PTSD. European Journal of Psychotraumatology, Volume 11, Issue 1, 2020.
2. Tapilskaya N.I., et al., Stress-protective effects of micronized progesterone in treatment of anxiety disorders in pregnant women after in vitro fertilization. Gynecology, Vol 23, No 4, 2021.
3. Watcharin N.Sovijit, et al., Ovarian progesterone suppresses depression and anxiety-like behaviors by increasing the Lactobacillus population of gut microbiota in ovariectomized mice. Neuroscience Research, Volume 168, 2021.
4. Mutakabbir Rashid Chowdhury, et al., Vitex peduncularis Boosted Anxiolytic, Antidepressant, and Antioxidant Properties in Albino Mice and In Silico Model. Journal of Herbs, Spices & Medicinal Plants, Volume 27, Issue 1, 2021.
Could Your Anxiety Be Related to Progesterone Levels? By Tara Peyman, ND
Anxiety is one of the most common mental health conditions. Feelings of anxiousness are normal for everyone to experience from time to time. However, for some people, anxiety can become severe and interruptive to daily functioning. This is when it is important to seek professional help and look for the underlying cause.
Sometimes anxiety is related to ongoing stress in your current daily life, and sometimes there is a history of trauma that has wired your nervous system to get stuck in a fight or flight state, leading to persistent anxiety even when there is nothing externally wrong in your current life to cause such high levels of anxiety. Stress and trauma tend to respond well to psychological therapy, such as CBT, EMDR, or other counseling modalities. Some people get great relief using natural supplements for stress reduction, such as passionflower, L-theanine, or homeopathic remedies.
Yet sometimes there is another cause. For females with anxiety, there can be a hormonal connection. If you notice that anxiety levels tend to fluctuate throughout the month, or if anxiety has been worse since menopausal changes, hormones may be at play here.
Progesterone can have a tranquilizing effect on the brain and nervous system. It does this primarily by acting on GABA receptors to calm the body and brain.1,2 Interestingly, there is a gut-brain connection with progesterone as well. Progesterone has been found to act as a probiotic in the digestive system, promoting growth of the beneficial bacteria, lactobacillus reuteri.3 This healthy bacteria strain has been shown to diminish anxiety levels and improve mental health.
If progesterone levels are relatively low, the nervous system may feel more stimulated, anxious, and restless. Some females with low progesterone will feel highly irritable as well. Low progesterone may lead to insomnia, which often happens during the luteal phase of a woman’s menstrual cycle, the phase when PMS is most likely to occur.
Progesterone also tends to drop first, before estrogen levels drop, during perimenopause. This means that females in their 40s and early 50s may start to have difficulty with insomnia, irritability, and anxiety, before they develop the classic menopausal symptoms of hot flashes and night sweats, which are more commonly related to a drop in estrogen.
If you are curious about whether progesterone might be a contributing factor in your anxiety, one good first step would be to make some notes about when anxiety occurs. Does there seem to be a cyclical pattern of anxiety or agitation increasing before your menstrual cycle? Has anxiety or insomnia increased or started as you’ve gotten older, possibly related to declining progesterone levels?
Most of the time, there are multiple factors that lead to heightened anxiety, and these factors play off of each other. For example, if your progesterone is lower, and you are not sleeping well and feeling anxious, you may be less productive at work or more irritable with others, and this can lead to increased stress and worry about these issues.
Stress and anxiety also can play a role in reducing progesterone levels, because progesterone is partly produced by the adrenal glands, and when you are under greater stress, your adrenal glands – the primary glands responsible for stress management in the body – will shunt more of their focus to production of cortisol and reduce focus on reproductive hormone production. So, in this way, there can be a cyclical effect of stress and anxiety causing low progesterone, which leads to more anxiety and stress.
How can we intervene to help this problem? Hormone testing is the first key element, to measure your levels of progesterone, estrogen, testosterone, cortisol, DHEA, thyroid hormones, vitamin D, and other markers that your doctor might be interested in testing, to get the whole picture of your internal health status. Once you have test results, your doctor can help determine whether there are imbalances between your hormones, or other issues that need to be addressed, in order to resolve the issues you are facing.
Treatment for progesterone deficiency may include herbal supplements, such as vitex, to promote more progesterone effects in the body. Vitex can also have specific antidepressant and anti-anxiety benefits, in addition to its hormone balancing effects, and was found to be similar in efficacy to fluoxetine in one study.4 If estrogen is relatively high and progesterone is normal or only slightly suboptimal, bringing the ratio into balance is key. This can be done with an estrogen reducing natural supplement, such as DIM (diindolylmethane) or I3C (indole-3-carbanol), both made from vegetable sources. For people with very low progesterone, or women further into perimenopause, progesterone supplementation may be a better option. This can take the form of low dose over-the-counter progesterone creams, or a bioidentical progesterone prescription from a pharmacy.
It is important to be well informed regarding all the risks and benefits of these treatment options, and to discuss them in detail with a doctor who is well versed in holistic hormone treatments. It is also vital to focus on the whole picture, because when it comes to hormonal health, balance is key. What is most important is to have the right ratios of each of the hormones, as well as a healthy diet and lifestyle that includes mindful self-care, to feel at your best.
References:
1. Antonia V. Seligowski, et al., Translational studies of estradiol and progesterone in fear and PTSD. European Journal of Psychotraumatology, Volume 11, Issue 1, 2020.
2. Tapilskaya N.I., et al., Stress-protective effects of micronized progesterone in treatment of anxiety disorders in pregnant women after in vitro fertilization. Gynecology, Vol 23, No 4, 2021.
3. Watcharin N.Sovijit, et al., Ovarian progesterone suppresses depression and anxiety-like behaviors by increasing the Lactobacillus population of gut microbiota in ovariectomized mice. Neuroscience Research, Volume 168, 2021.
4. Mutakabbir Rashid Chowdhury, et al., Vitex peduncularis Boosted Anxiolytic, Antidepressant, and Antioxidant Properties in Albino Mice and In Silico Model. Journal of Herbs, Spices & Medicinal Plants, Volume 27, Issue 1, 2021.
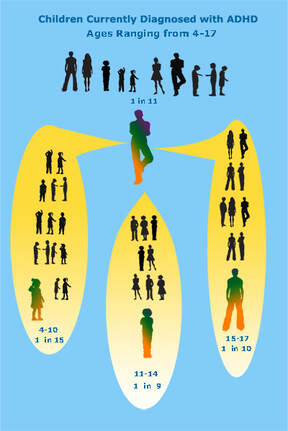 Image by CHADD.ORG
Image by CHADD.ORG
8/3/2022
ADHD vs. Anxiety in Kids By Hillary Lim ND
It’s that time of year again. . . back to school! As your child is entering a new year, or perhaps starting school for the first time, there may be some of you who are concerned about your child’s ability to function optimally at school. Maybe they struggle with sitting still, focusing, or have the tendency to be disruptive or forgetful. You may be thinking, “Does my child have ADHD? Or is he/she just an anxious little human?”. Hopefully this article will help to guide you in identifying what’s going on with your child so you can take some helpful action steps in this new school year!
Let’s start with some data. According to the CDC, 6.1 million children have been diagnosed with ADHD in the U.S., with 1 in 9 children diagnosed with ADHD between the ages of 11 - 14.
But how do you know if you should have your child evaluated for ADHD? The first step is to refer to the diagnostic guidelines for ADHD (please take a moment to scroll down to the end of the article to refer to the diagnostic criteria.)
Come back here to continue reading!
Now that you’ve gone through the diagnostic guidelines, you should have a better idea of whether or not your child may have ADHD. The next question is, if my child does meet the above criteria, do I need to get him/her officially evaluated? If you feel like your child would benefit from accommodations at school, like extra time for testing, a wiggle chair, one-on-one tutoring if provided, etc. then yes! They will need to be evaluated by a provider like a psychiatrist or developmental pediatrician to be officially diagnosed. Then you can take that diagnostic evaluation to the school and set up an Individualized Education Plan (IEP) for your child to help them to be as successful as possible at school!
The next question is, what do I do if my child does have ADHD? Most people are familiar with the traditional medication options for ADHD, which include both stimulant and non-stimulant meds. However, many parents would prefer to try more natural ways to address the symptoms before going down the medication road. Every individual is different, but for many children there are ways to improve in areas like focus, restlessness, and working memory without the use of traditional medications. Individualized combinations of various therapies like homeopathic treatment, gut healing protocols, hormone and nutrient balancing, detoxification, Craniosacral therapy, neurofeedback, and nutritional supplements are key to optimizing brain function and focus! It’s also important for kids with ADHD to learn about how special they are, their strengths, and their weaknesses so they can learn skills that they can use throughout their life which will help them to maintain balance as much as possible.
Now, what if your child doesn’t exactly meet enough of the criteria for ADHD above, but there are still prevalent symptoms that are affecting everyday life?
Could it be Anxiety?
Sometimes what presents as ADHD is actually anxiety! Kids don’t always know how to verbalize their stress and worry, so they may exhibit one or more of the following symptoms:
It’s also possible that your child has BOTH ADHD and anxiety. If you’re feeling overwhelmed, just remember that there are action steps to take that don’t involve prescription medications!
The first step is getting a holistic workup done. Ideally, this would involve ordering diagnostic blood/urine tests. This allows us to investigate if there is a physiological reason that the symptoms are there so we can address that physiological imbalance.
Common abnormal lab results in kids with ADHD/anxiety/or both!
Another important part of the workup should be identifying any anxiety symptoms or other physical symptoms that are there. Connecting kids with their own bodies and helping them to identify their emotions and sensations is very important. If they still don’t have the words to describe the emotion or sensation in detail, that’s OK! They will still be able to give us some basic insight. For example, “My tummy hurts when I think about school” or “When I try to go to sleep it feels like there’s ants crawling up and down my legs”. Then we can use that information to help to decrease the prevalence of that symptom, by using things like homeopathy, individualized guided meditations, tapping techniques, etc.
Natural Treatment Options
Again, most people are aware of the medication avenue for ADHD and anxiety. If you are interested in a more holistic approach, there are options out there! I would recommend finding a Naturopathic Doctor (N.D. or N.M.D. depending on the state you live in) to help address the underlying imbalances and tendencies that are contributing to the symptoms that are present. He/she can help you in various ways by recommending one, a few, or all of the following:
At IMHC, all of our doctors are familiar with treating both ADHD and anxiety in kids. We can see individuals locally in AZ, and can act as naturopathic consultants for individuals living out of the state or country. To schedule your free phone consult with IMHC’s medical director, click here.
Resources:
“General Prevalence of ADHD”, Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD), Accessed August 3, 2022, https://chadd.org/about-adhd/general-prevalence/
“ADHD19 Assessment Table”, American Academy of Family Physicians, Accessed August 3, 2022, https://www.aafp.org/dam/AAFP/documents/patient_care/adhd_toolkit/adhd19-assessment-table1.pdf
ADHD vs. Anxiety in Kids By Hillary Lim ND
It’s that time of year again. . . back to school! As your child is entering a new year, or perhaps starting school for the first time, there may be some of you who are concerned about your child’s ability to function optimally at school. Maybe they struggle with sitting still, focusing, or have the tendency to be disruptive or forgetful. You may be thinking, “Does my child have ADHD? Or is he/she just an anxious little human?”. Hopefully this article will help to guide you in identifying what’s going on with your child so you can take some helpful action steps in this new school year!
Let’s start with some data. According to the CDC, 6.1 million children have been diagnosed with ADHD in the U.S., with 1 in 9 children diagnosed with ADHD between the ages of 11 - 14.
But how do you know if you should have your child evaluated for ADHD? The first step is to refer to the diagnostic guidelines for ADHD (please take a moment to scroll down to the end of the article to refer to the diagnostic criteria.)
Come back here to continue reading!
Now that you’ve gone through the diagnostic guidelines, you should have a better idea of whether or not your child may have ADHD. The next question is, if my child does meet the above criteria, do I need to get him/her officially evaluated? If you feel like your child would benefit from accommodations at school, like extra time for testing, a wiggle chair, one-on-one tutoring if provided, etc. then yes! They will need to be evaluated by a provider like a psychiatrist or developmental pediatrician to be officially diagnosed. Then you can take that diagnostic evaluation to the school and set up an Individualized Education Plan (IEP) for your child to help them to be as successful as possible at school!
The next question is, what do I do if my child does have ADHD? Most people are familiar with the traditional medication options for ADHD, which include both stimulant and non-stimulant meds. However, many parents would prefer to try more natural ways to address the symptoms before going down the medication road. Every individual is different, but for many children there are ways to improve in areas like focus, restlessness, and working memory without the use of traditional medications. Individualized combinations of various therapies like homeopathic treatment, gut healing protocols, hormone and nutrient balancing, detoxification, Craniosacral therapy, neurofeedback, and nutritional supplements are key to optimizing brain function and focus! It’s also important for kids with ADHD to learn about how special they are, their strengths, and their weaknesses so they can learn skills that they can use throughout their life which will help them to maintain balance as much as possible.
Now, what if your child doesn’t exactly meet enough of the criteria for ADHD above, but there are still prevalent symptoms that are affecting everyday life?
Could it be Anxiety?
Sometimes what presents as ADHD is actually anxiety! Kids don’t always know how to verbalize their stress and worry, so they may exhibit one or more of the following symptoms:
- Forgetfulness
- Restlessness
- Excessive worry about school or social situations
- Overly clingy
- Sleep difficulties
- Struggling with focus
- Talking rapidly
- Irritability
- Stomach aches
It’s also possible that your child has BOTH ADHD and anxiety. If you’re feeling overwhelmed, just remember that there are action steps to take that don’t involve prescription medications!
The first step is getting a holistic workup done. Ideally, this would involve ordering diagnostic blood/urine tests. This allows us to investigate if there is a physiological reason that the symptoms are there so we can address that physiological imbalance.
Common abnormal lab results in kids with ADHD/anxiety/or both!
- Anemia (too little iron, B12, folate, or all of the above!)
- Genetic methylation difficulties
- Yeast overgrowth in the gut
- Decreased mitochondrial function
- Lead toxicity
- Vitamin D deficiency
- Thyroid and/or adrenal function disturbance
- Difficulty with processing histamines
Another important part of the workup should be identifying any anxiety symptoms or other physical symptoms that are there. Connecting kids with their own bodies and helping them to identify their emotions and sensations is very important. If they still don’t have the words to describe the emotion or sensation in detail, that’s OK! They will still be able to give us some basic insight. For example, “My tummy hurts when I think about school” or “When I try to go to sleep it feels like there’s ants crawling up and down my legs”. Then we can use that information to help to decrease the prevalence of that symptom, by using things like homeopathy, individualized guided meditations, tapping techniques, etc.
Natural Treatment Options
Again, most people are aware of the medication avenue for ADHD and anxiety. If you are interested in a more holistic approach, there are options out there! I would recommend finding a Naturopathic Doctor (N.D. or N.M.D. depending on the state you live in) to help address the underlying imbalances and tendencies that are contributing to the symptoms that are present. He/she can help you in various ways by recommending one, a few, or all of the following:
- Homeopathic Treatment
- Craniosacral Therapy
- Gut testing and gut healing protocols
- Detoxification Protocols
- Neurofeedback
- Cognitive Behavioral Therapy
- Nutritional Supplementation to address underlying deficiencies
- Genetic testing and support
- Other possible learning disability support
At IMHC, all of our doctors are familiar with treating both ADHD and anxiety in kids. We can see individuals locally in AZ, and can act as naturopathic consultants for individuals living out of the state or country. To schedule your free phone consult with IMHC’s medical director, click here.
Resources:
“General Prevalence of ADHD”, Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD), Accessed August 3, 2022, https://chadd.org/about-adhd/general-prevalence/
“ADHD19 Assessment Table”, American Academy of Family Physicians, Accessed August 3, 2022, https://www.aafp.org/dam/AAFP/documents/patient_care/adhd_toolkit/adhd19-assessment-table1.pdf
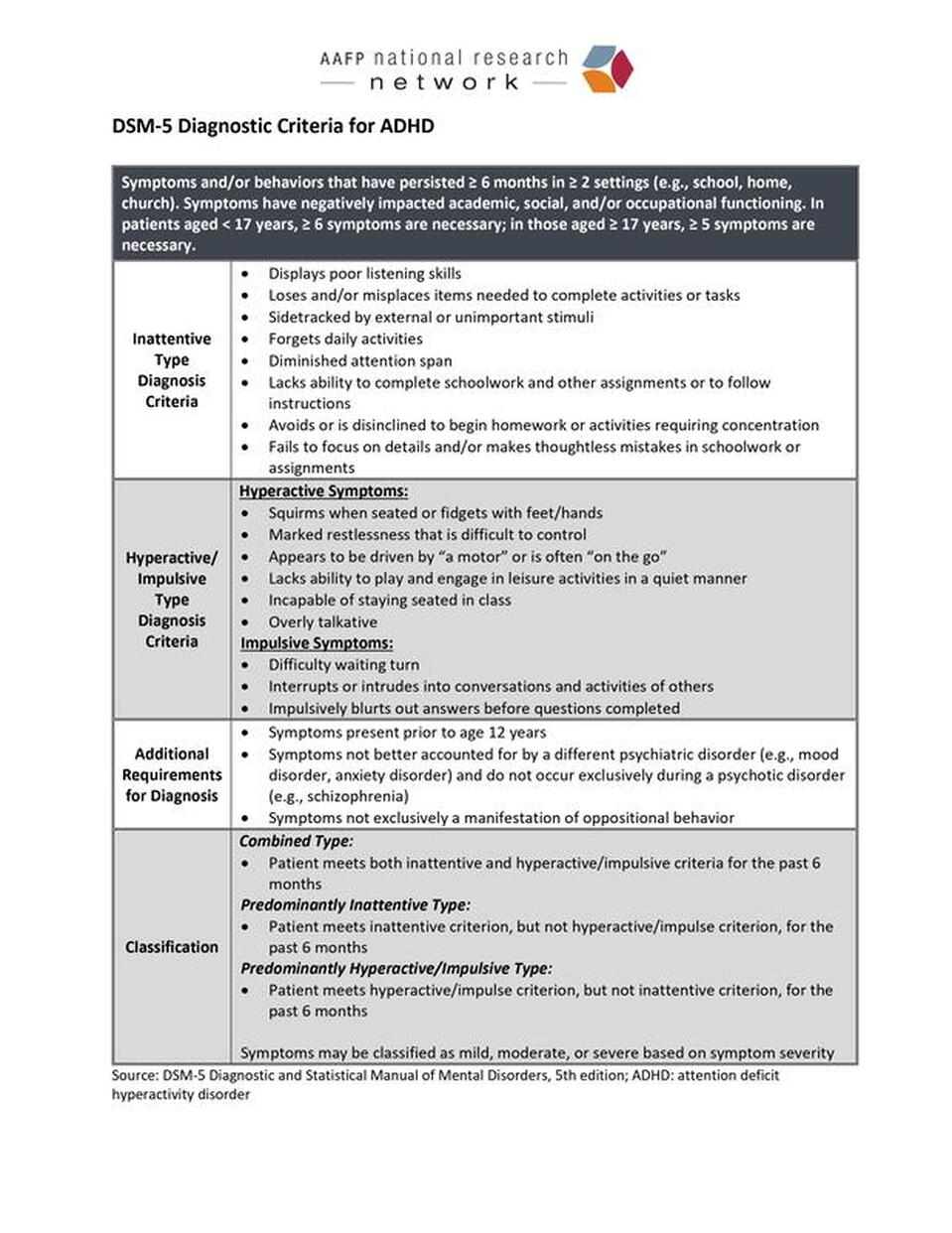
Image by AAFP.ORG
6/28/22
Disparities in Racial/Ethnic Minority Mental Health
By Molly Tately, ND
July marks National Minority Mental Health Awareness Month, highlighting the unique challenges encountered by racial and ethnic minorities regarding mental health in the United States. According to the Substance Abuse and Mental Health Services Administration’s (SAMHSA) 2020 National Survey on Drug Use and Health, 52.9 million adults in the United States suffer from a mental, behavioral, or emotional disorder. An estimated 49.5% of adolescents aged 13-18 have had a mental disorder at some point in their life.1
Based upon SAMHSA’s survey, racial/ethnic minority groups tend to have fewer mental health disorders than White individuals. This has long been the case and is something that researchers have struggled to explain as American social environments largely seem less than conducive to supporting the mental health of our minority populations. The risk factors for development of mental health disorders are immense. The original CDC-Kaiser Adverse Childhood Experiences (ACE) Study published in 1998 established a strong basis of understanding of this by looking at seven domains: physical/emotional/sexual abuse, household mental illness, household substance use, household domestic violence, and incarcerated household member.2 (Parental separation/divorce was later added as an eighth domain in subsequent studies.) Frequencies of adverse experiences were calculated by domain and a mean ACE score determined. Exposure to events in these domains showed significant physical health risks, but also strong links to depression, anxiety, severe mood disorders, and suicide with a higher ACE score correlating to higher risk for poor physical and mental health. The 2020 data shows that White individuals had lower mean ACE scores (1.53) than Black (1.66) or Hispanic (1.63) individuals.3 This demonstrates a tremendous amount of stress on these racial/ethnic minorities, putting them at higher risk for mental illness.
Underestimating and under-reporting in minority group mental illness has been suggested as a rationale for the above-mentioned minority mental health paradox.4,5 Differences in conceptualization of mental illness has also been postulated. One study offered that “holistic cultures” rooted in Buddhism, Confucianism, Hinduism, and Taoism acted as a protective factor against the development of mental disorders. These cultures were assessed to have lower expectations for ideal levels of happiness, health, and self-esteem and therefore interpret negative experiences in a more neutral manner than individualistic cultures like the United States.4 While possibly explaining a factor involved in prevalence disparities in the Asian minority population, this cultural basis doesn’t appear to apply across all other racial/ethnic minority groups of the United States which also demonstrate lower rates of mental illness.
A recent study out of the University of Pennsylvania took another approach and explored frequently prescribed medications for physical health conditions such as certain analgesics, antihypertensives, corticosteroids, gastrointestinal agents, hormone modifiers, and respiratory agents with depression or suicide as side-effects. Large differences in the use of pharmaceutical medications along racial/ethnic lines were identified according to analysis of data in the Medical Expenditure Panel Survey (MEPS). 37% of adults in the United States currently take at least one medication with these adverse effects and 15% take three or more.5 Of these, White individuals consumed higher levels of medications with side effects of depression or suicide (28%) than individuals in any other ethnic/racial group (no higher than 15%).5 Analysis revealed that taking even a single medication with suicide as a possible side-effect more than doubled the chance of mental/emotional disturbance; taking three or more further compounded this further. Interestingly, it is the decreased utilization of pharmaceutical interventions for physical health conditions that appears to be a potentially protective factor for racial/ethnic minorities against the development of mental disorders. This observation leads to more questions as improved physical health has historically been correlated with improved mental health.
Lower levels of minority service utilization are not limited to just the physical health space. Racial/ethnic minorities diagnosed with mental illness are less likely to receive mental health services to address their conditions. In 2020, 46.2% of adults with any mental illness received mental health services including inpatient treatment, outpatient treatment/counseling, or prescription medication(s).1 Of these, White individuals were most likely to receive treatment (51.8%), whereas only 20.8% of Asian individuals, 35.1% of Hispanic individuals, and 37.1% of Black individuals received care.1 Differences along racial/ethnic lines were also identified in the types of services accessed more frequently. White and American Indian/Alaska Native individuals were more likely to receive outpatient mental health services and take prescription psychiatric medications and Black individuals were more likely to receive inpatient mental health services.6 A study by Hudson et al revealed that White children are about twice as likely as Black or Hispanic children to be treated with stimulant medications for attention deficit/hyperactivity disorder.7 Similarly, White adolescents are about twice as likely as Hispanic adolescents to be treated with antidepressant medications.8
The American Psychiatric Association cites multiple factors for the disparity in mental health service provision and poorer outcomes amongst racial/ethnic minorities. These include inaccessibility of high-quality mental health care services, cultural stigma surrounding mental health care, discrimination, and overall lack of awareness about mental health.9 Language challenges, lack of diversity among mental health care providers, lack of culturally competent providers, and distrust of the healthcare system were also identified as barriers.6 Some evidence suggests apprehension surrounding common interventions targeted at addressing mental disorders is also a factor. For example, Black and Hispanic patients express higher concerns than White patients about side-effects and quality of life effects of pharmaceuticals.7 And finally, higher ACEs may affect attitudes about health and healthcare in general which could reasonably impact service utilization.2
Studies also suggest that incidents of racial discrimination are of profound importance for mental health because they are “experiences of exclusion that trigger feelings of a ‘defilement of self.’ This includes feelings of being over-scrutinized, overlooked, underappreciated, misunderstood, and disrespected.”10 These, like ACEs, can lead to heightened vigilance through both actual exposure or even the threat of exposure to a potentially discriminatory experience. This is an important consideration within the context of mental healthcare where the quality of patient-provider interactions is critical to developing a positive therapeutic relationship.
Here at IMHC we acknowledge the importance of our patients’ lived experiences and focus on each individual holistically. We work collaboratively with our patients in putting together their treatment plans and choosing an array of natural and conventional therapeutic options to address both mental and underlying physical health concerns. We have doctors that speak Spanish and Korean and work with translators as needed to include individuals where language may be a barrier to receiving care.
References
Disparities in Racial/Ethnic Minority Mental Health
By Molly Tately, ND
July marks National Minority Mental Health Awareness Month, highlighting the unique challenges encountered by racial and ethnic minorities regarding mental health in the United States. According to the Substance Abuse and Mental Health Services Administration’s (SAMHSA) 2020 National Survey on Drug Use and Health, 52.9 million adults in the United States suffer from a mental, behavioral, or emotional disorder. An estimated 49.5% of adolescents aged 13-18 have had a mental disorder at some point in their life.1
Based upon SAMHSA’s survey, racial/ethnic minority groups tend to have fewer mental health disorders than White individuals. This has long been the case and is something that researchers have struggled to explain as American social environments largely seem less than conducive to supporting the mental health of our minority populations. The risk factors for development of mental health disorders are immense. The original CDC-Kaiser Adverse Childhood Experiences (ACE) Study published in 1998 established a strong basis of understanding of this by looking at seven domains: physical/emotional/sexual abuse, household mental illness, household substance use, household domestic violence, and incarcerated household member.2 (Parental separation/divorce was later added as an eighth domain in subsequent studies.) Frequencies of adverse experiences were calculated by domain and a mean ACE score determined. Exposure to events in these domains showed significant physical health risks, but also strong links to depression, anxiety, severe mood disorders, and suicide with a higher ACE score correlating to higher risk for poor physical and mental health. The 2020 data shows that White individuals had lower mean ACE scores (1.53) than Black (1.66) or Hispanic (1.63) individuals.3 This demonstrates a tremendous amount of stress on these racial/ethnic minorities, putting them at higher risk for mental illness.
Underestimating and under-reporting in minority group mental illness has been suggested as a rationale for the above-mentioned minority mental health paradox.4,5 Differences in conceptualization of mental illness has also been postulated. One study offered that “holistic cultures” rooted in Buddhism, Confucianism, Hinduism, and Taoism acted as a protective factor against the development of mental disorders. These cultures were assessed to have lower expectations for ideal levels of happiness, health, and self-esteem and therefore interpret negative experiences in a more neutral manner than individualistic cultures like the United States.4 While possibly explaining a factor involved in prevalence disparities in the Asian minority population, this cultural basis doesn’t appear to apply across all other racial/ethnic minority groups of the United States which also demonstrate lower rates of mental illness.
A recent study out of the University of Pennsylvania took another approach and explored frequently prescribed medications for physical health conditions such as certain analgesics, antihypertensives, corticosteroids, gastrointestinal agents, hormone modifiers, and respiratory agents with depression or suicide as side-effects. Large differences in the use of pharmaceutical medications along racial/ethnic lines were identified according to analysis of data in the Medical Expenditure Panel Survey (MEPS). 37% of adults in the United States currently take at least one medication with these adverse effects and 15% take three or more.5 Of these, White individuals consumed higher levels of medications with side effects of depression or suicide (28%) than individuals in any other ethnic/racial group (no higher than 15%).5 Analysis revealed that taking even a single medication with suicide as a possible side-effect more than doubled the chance of mental/emotional disturbance; taking three or more further compounded this further. Interestingly, it is the decreased utilization of pharmaceutical interventions for physical health conditions that appears to be a potentially protective factor for racial/ethnic minorities against the development of mental disorders. This observation leads to more questions as improved physical health has historically been correlated with improved mental health.
Lower levels of minority service utilization are not limited to just the physical health space. Racial/ethnic minorities diagnosed with mental illness are less likely to receive mental health services to address their conditions. In 2020, 46.2% of adults with any mental illness received mental health services including inpatient treatment, outpatient treatment/counseling, or prescription medication(s).1 Of these, White individuals were most likely to receive treatment (51.8%), whereas only 20.8% of Asian individuals, 35.1% of Hispanic individuals, and 37.1% of Black individuals received care.1 Differences along racial/ethnic lines were also identified in the types of services accessed more frequently. White and American Indian/Alaska Native individuals were more likely to receive outpatient mental health services and take prescription psychiatric medications and Black individuals were more likely to receive inpatient mental health services.6 A study by Hudson et al revealed that White children are about twice as likely as Black or Hispanic children to be treated with stimulant medications for attention deficit/hyperactivity disorder.7 Similarly, White adolescents are about twice as likely as Hispanic adolescents to be treated with antidepressant medications.8
The American Psychiatric Association cites multiple factors for the disparity in mental health service provision and poorer outcomes amongst racial/ethnic minorities. These include inaccessibility of high-quality mental health care services, cultural stigma surrounding mental health care, discrimination, and overall lack of awareness about mental health.9 Language challenges, lack of diversity among mental health care providers, lack of culturally competent providers, and distrust of the healthcare system were also identified as barriers.6 Some evidence suggests apprehension surrounding common interventions targeted at addressing mental disorders is also a factor. For example, Black and Hispanic patients express higher concerns than White patients about side-effects and quality of life effects of pharmaceuticals.7 And finally, higher ACEs may affect attitudes about health and healthcare in general which could reasonably impact service utilization.2
Studies also suggest that incidents of racial discrimination are of profound importance for mental health because they are “experiences of exclusion that trigger feelings of a ‘defilement of self.’ This includes feelings of being over-scrutinized, overlooked, underappreciated, misunderstood, and disrespected.”10 These, like ACEs, can lead to heightened vigilance through both actual exposure or even the threat of exposure to a potentially discriminatory experience. This is an important consideration within the context of mental healthcare where the quality of patient-provider interactions is critical to developing a positive therapeutic relationship.
Here at IMHC we acknowledge the importance of our patients’ lived experiences and focus on each individual holistically. We work collaboratively with our patients in putting together their treatment plans and choosing an array of natural and conventional therapeutic options to address both mental and underlying physical health concerns. We have doctors that speak Spanish and Korean and work with translators as needed to include individuals where language may be a barrier to receiving care.
References
- Mental illness. National Institute of Mental Health. https://www.nimh.nih.gov/health/statistics/mental-illness. Accessed June 23, 2022.
- Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. Am J Prev Med. 1998;14(4):245-258. doi:10.1016/s0749-3797(98)00017-8
- Giano Z, Wheeler DL, Hubach RD. The frequencies and disparities of adverse childhood experiences in the U.S. BMC Public Health. 2020;20(1):1327. Published 2020 Sep 10. doi:10.1186/s12889-020-09411-z
- Alvarez K, Fillbrunn M, Green JG, et al. Race/ethnicity, nativity, and lifetime risk of mental disorders in US adults. Soc Psychiatry Psychiatr Epidemiol. 2019;54(5):553-565. doi:10.1007/s00127-018-1644-5
- Schnittker J, Do D. Pharmaceutical Side Effects and Mental Health Paradoxes among Racial-Ethnic Minorities. J Health Soc Behav. 2020;61(1):4-23. doi:10.1177/0022146519899115
- Mental health disparities: Diverse populations. https://www.psychiatry.org/File%20Library/Psychiatrists/Cultural-Competency/Mental-Health-Disparities/Mental-Health-Facts-for-Diverse-Populations.pdf. Accessed June 20, 2022.
- Hudson JL, Miller GE, Kirby JB. Explaining racial and ethnic differences in children's use of stimulant medications. Med Care. 2007;45(11):1068-1075. doi:10.1097/MLR.0b013e31806728fa
- Mental health disparities: Hispanics and Latinos. https://www.psychiatry.org/File%20Library/Psychiatrists/Cultural-Competency/Mental-Health-Disparities/Mental-Health-Facts-for-Hispanic-Latino.pdf. Accessed June 27, 2022.
- Mental health disparities: Diverse populations. Psychiatry.org - Mental Health Disparities: Diverse Populations. https://www.psychiatry.org/psychiatrists/cultural-competency/education/mental-health-facts. Accessed June 20, 2022.
- Williams DR. Stress and the Mental Health of Populations of Color: Advancing Our Understanding of Race-related Stressors. J Health Soc Behav. 2018;59(4):466-485. doi:10.1177/0022146518814251
4/5/2022
Craniosacral Q & A with Dr. Hillary Lim, N.D.
How long have you been practicing Craniosacral Therapy?
I have been a Craniosacral Therapist for close to 10 years. I have performed CST at least 4,500 times and have loved every minute of it!
What led you to become a Craniosacral Therapist?
I first chose to learn this modality from the Upledger Institute as I was looking for a gentle way to work on babies and small children that was different from the high velocity manipulations that we learned in medical school. I didn’t fully understand the vast benefits that Craniosacral can provide when I first started. We were of course introduced to the many conditions that benefit from this type of work, but it wasn’t until I started the work in my own practice that I fully understood the changes that Craniosacral Therapy can bring about.
What are your favorite conditions to treat?
That’s a hard one! I love treating common physical ailments like migraines, TMJ, vertigo, back pain, and constipation. But I also love working on the nervous system in individuals with anxiety, insomnia and PTSD.
What should people expect at their first session?
This varies based on the condition and age of the patient, but generally people feel very relaxed during and after their session. Some people may feel more emotional that day as the body is clearing things, some people feel tired and want to take a nap, and others feel lighter and more energized. This can also vary from session to session, based on what happened on my treatment table that day! I always encourage people to drink extra water after the session to help to clear any toxins (physical and emotional!) that may have been released that day.
Can you share a recent success story?
Of course! I’ll tell you two that just came to mind! One was in regards to an infant who was waking every 2 hours at night and crying (mom and dad were VERY tired!). He was also only having a BM once every 7-10 days! Poor guy. He started having more frequent BM’s even after the first treatment and now is sleeping well, is having BM’s 1-3 times daily, and is an overall happier little guy (and mom and dad are finally getting some rest!)
Another story is in regards to a young woman who suffers from PTSD. While we were doing Craniosacral Therapy she had some old trauma come to the surface and she was able to release some of the fear and anger that she had been storing inside of her. After the session she felt lighter and more relaxed and left my office with a big sigh of relief.
Click here for more information about Craniosacral Therapy
Craniosacral Q & A with Dr. Hillary Lim, N.D.
How long have you been practicing Craniosacral Therapy?
I have been a Craniosacral Therapist for close to 10 years. I have performed CST at least 4,500 times and have loved every minute of it!
What led you to become a Craniosacral Therapist?
I first chose to learn this modality from the Upledger Institute as I was looking for a gentle way to work on babies and small children that was different from the high velocity manipulations that we learned in medical school. I didn’t fully understand the vast benefits that Craniosacral can provide when I first started. We were of course introduced to the many conditions that benefit from this type of work, but it wasn’t until I started the work in my own practice that I fully understood the changes that Craniosacral Therapy can bring about.
What are your favorite conditions to treat?
That’s a hard one! I love treating common physical ailments like migraines, TMJ, vertigo, back pain, and constipation. But I also love working on the nervous system in individuals with anxiety, insomnia and PTSD.
What should people expect at their first session?
This varies based on the condition and age of the patient, but generally people feel very relaxed during and after their session. Some people may feel more emotional that day as the body is clearing things, some people feel tired and want to take a nap, and others feel lighter and more energized. This can also vary from session to session, based on what happened on my treatment table that day! I always encourage people to drink extra water after the session to help to clear any toxins (physical and emotional!) that may have been released that day.
Can you share a recent success story?
Of course! I’ll tell you two that just came to mind! One was in regards to an infant who was waking every 2 hours at night and crying (mom and dad were VERY tired!). He was also only having a BM once every 7-10 days! Poor guy. He started having more frequent BM’s even after the first treatment and now is sleeping well, is having BM’s 1-3 times daily, and is an overall happier little guy (and mom and dad are finally getting some rest!)
Another story is in regards to a young woman who suffers from PTSD. While we were doing Craniosacral Therapy she had some old trauma come to the surface and she was able to release some of the fear and anger that she had been storing inside of her. After the session she felt lighter and more relaxed and left my office with a big sigh of relief.
Click here for more information about Craniosacral Therapy
Videos
Dr. Tara Peyman, our Clinical Director and go-to expert for schizophrenia and bipolar disorder, discusses using homeopathy for mental illness below:
Our owner and expert in autism and mood disorders, Dr. Hillary Lim, discusses how to naturally increase beneficial neurotransmitters below:
A video created by a client that has worked with Dr. Peyman, discussing the benefits of homeopathic and naturopathic treatment options in the treatment of mental health conditions. This video was created by Deb Cross from Celebrate Your Life Studio.